February 26, 2026 | Nerve Pain
2 minute read

Over the years, this question has arisen with some regularity, and the explanation is relatively straightforward although it requires some nuance. Consider an arbitrary area of skin or scalp that is innervated by three separate sensory nerves.
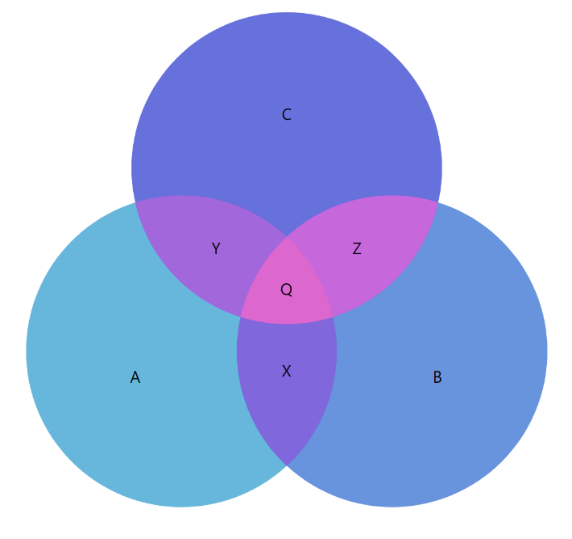
In practical terms, this means that all three nerves contribute to sensation in the same region of skin. When that area is touched, each nerve participates to some extent in transmitting the sensory signal. Because these nerves branch and interconnect within the tissue, their sensory territories often overlap rather than existing as sharply defined, isolated zones – much like overlapping regions in a Venn diagram (see area ‘Q’ in the diagram below).
Now assume that one of these three nerves becomes injured and begins generating pain. If a surgical procedure is performed in which the injured nerve is transected and managed appropriately, the goal is to reduce or eliminate the aberrant pain signaling over time. Importantly, however, the remaining two nerves continue to supply sensation to that same patch of skin. As a result, when the patient touches the area after recovery, perception of touch is often largely preserved. The patient does not consciously distinguish which specific nerve is mediating the sensation and functionally, that distinction is irrelevant. What matters is that meaningful sensation remains while the painful input from the injured nerve has been addressed.
This concept of overlapping sensory territories also helps explain why patients can tolerate transection of certain sensory nerves without experiencing significant numbness. It is not the sole factor to consider when determining whether a nerve can be safely transected, but it is an important anatomical and physiological principle that informs surgical decision-making. That is why an evaluation by and conversation with an experienced peripheral nerve surgeon is so important.